Occlusion is a manner in which the teeth in the mandibular arch intercuspate with the teeth in the maxillary arch in any functional relation. An ideal occlusion is rarely found in nature. An individual’s occlusal status is generally described by two major characteristics: intra-arch relationship, the relationship of the teeth within each arch to a smoothly curving line of occlusion and inter-arch relationship, the pattern of occlusal contacts between the upper and lower teeth[1].
What is a malocclusion?
Edward Angle, widely recognized as the father of contemporary orthodontics introduced the initial classification system for malocclusion. Malocclusion indicates the misalignment or incorrect positioning of teeth when the jaws close, deviating from their normal relationship, and may or may not be accompanied by irregularities in the teeth. It is an appreciable deviation from the ideal occlusion that may be considered aesthetically unsatisfactory and may vary from mild to severe depending on age and ethnicity[2]. It is important to understand that not all deviations from normal or ideal occlusion require treatment; therefore the determination of treatment necessity is made after considering the function, potential oral health risks, facial balance, patient satisfaction and aesthetics. Today malocclusion occurs in the majority of the population[3].
How is malocclusion classified?
The classification of malocclusion is determined by the position and alignment of the teeth and jaw bones jaws observed from transverse, vertical and sagittal planes. Angle’s classifications rely on the position of the permanent maxillary first molar in centric occlusion, if they are missing, the canine’s position is used to determine the classification. The occlusion traits were assessed as normal occlusion or malocclusion using the first permanent molars as described by E.H. Angle and deviation from line of occlusion.[4]
What is the line of occlusion?
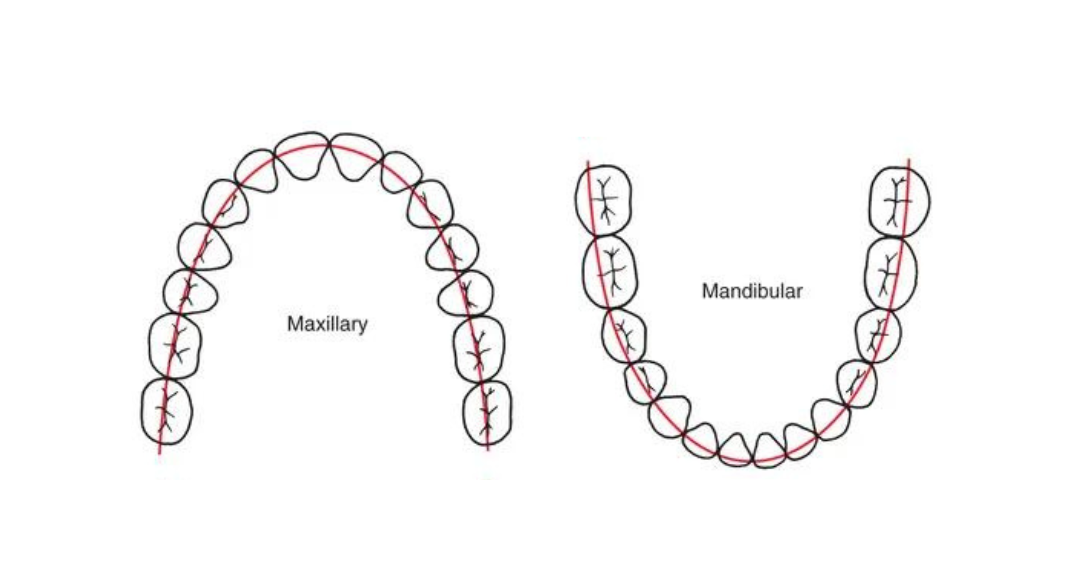
Ideally, all teeth should align along a line of occlusion with a normal overbite, overjet and coincident maxillary and mandibular midlines. The line of occlusion is characterized by a smooth curve that passes through the central fossae of the maxillary posterior teeth and across the cingulum of the upper anterior teeth. Similarly, it extends along the buccal cusps of the mandibular posterior teeth and the incisal edges of the lower anterior teeth.
What are the classifications of malocclusion?
In accordance with Angle’s classification, three classes of malocclusion were established based on the relationship of the mesiobuccal cusp of the maxillary first molar to the buccal groove of the mandibular first molar. The three classifications are:
- Class I: Also known as neutroocclusion, class I molar relationship refers to the proper occlusion of the mesiobuccal cusp of the maxillary first permanent molar to the buccal groove of the mandibular first permanent molar. Similarly, a class I canine relationship is characterized by the upper canine cusp resting in the embrasure between the lower canine and first premolar. Normal occlusion and Class I malocclusion shared the same molar relationship but differed in the arrangement of the teeth relative to the line of occlusion[5]. Class I might not have good alignment of teeth relative to the line of occlusion[6] as a result of crowding, misalignment in the teeth, rotations, or certain discrepancies in the upper and lower arches.

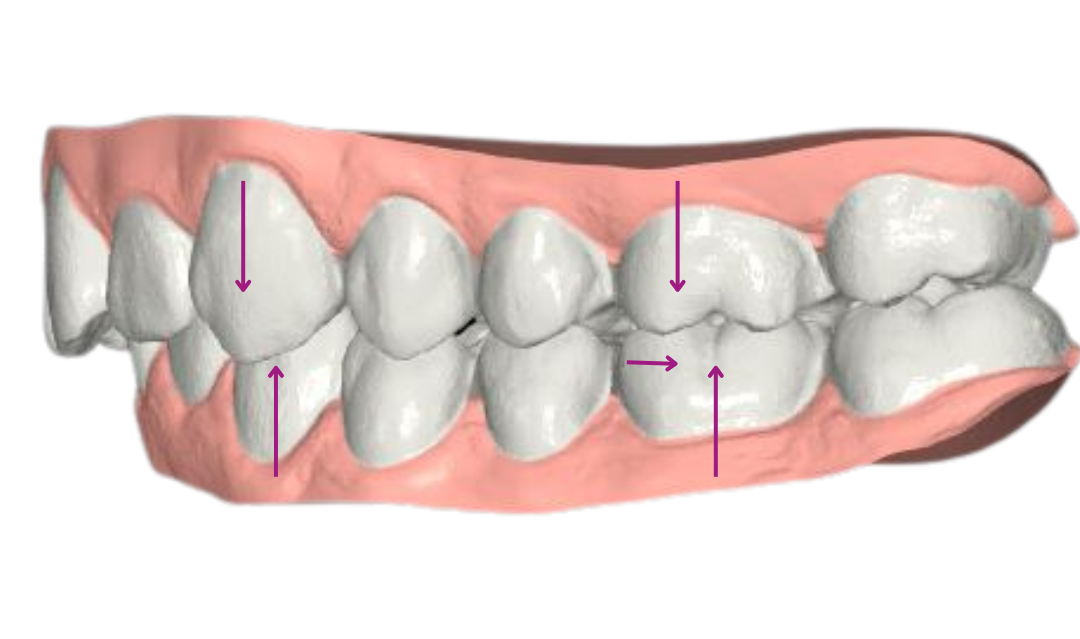
- Class II: Also known as distoocclusion, Class II molar relationship refers to the distal position of the mesiobuccal groove of the mandibular first permanent molar when in occlusion with the mesiobuccal cusp of the maxillary first permanent molar. Similarly, we are dealing with a Class II canine relationship if the cusp of the upper canine is positioned anteriorly to the embrasure between the lower canine and first premolar. In this case, the line of occlusion is not specified as it may or may not be irregular, it is influenced by factors such as the individual's facial pattern, overcrowding, and spacing requirements. Class II can be further differentiated into division 1 and division 2, which describe the relationship of the anterior teeth[7].
Class II division 1: In the case of Class II molar relation with protruded maxillary anterior teeth and large overjet[8].
Class II division 2: In the case of retroclined maxillary central incisors, proclined or normally inclined maxillary lateral incisors, and deep overbite[9].
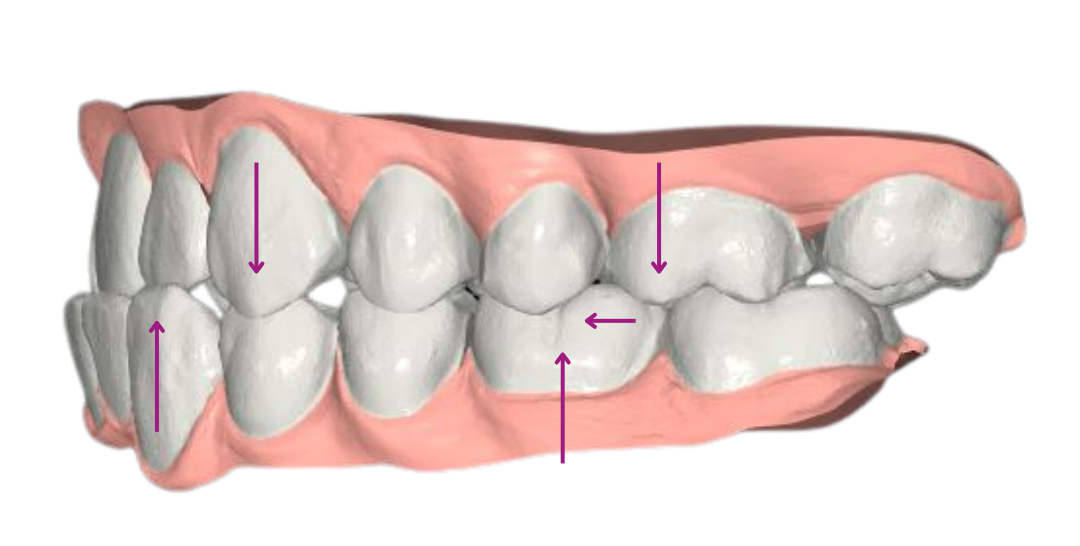
- Class III: Also known as mesioocclusion, class III molar relationship is observed when the mesiobuccal cusp of the maxillary first permanent molar occludes distally to the mesiobuccal groove of the mandibular permanent first molar. Similarly, the cusp of the upper canine is distally positioned to the embrasure between the lower canine and lower first premolar. The occlusion with Class III molar relation with pre-mature contact of incisors or the canines with or without negative overjet was classified as Class III malocclusion[10]. Class III malocclusions can be divided into two categories:
Skeletal class III: Genetic in nature, this condition arises due to an excessively large mandible or a smaller than average maxilla, leading to improper positioning of the entire jaw.
Dental class III: In pseudo-Class III malocclusion, the patient has normal maxilla and mandible sizes and has skeletal Class I malocclusion[11], however, the lower teeth are anteriorly positioned when compared to the upper teeth.
NB: When the molar is Class I on one side, and either Class II or III on the other side, the malocclusion is classified as a subdivision. The subdivision refers to the side that is either Class II or III[12].
What are some of the orthodontic methods that can be used for malocclusion correction?
Malocclusions become obvious as the child enters the phase of mixed dentition. They can be caused by habits like tongue habits, thumb sucking, mouth breathing...which can change the facial structures. The following appliances are some that are used by orthodontists to treat malocclusion:
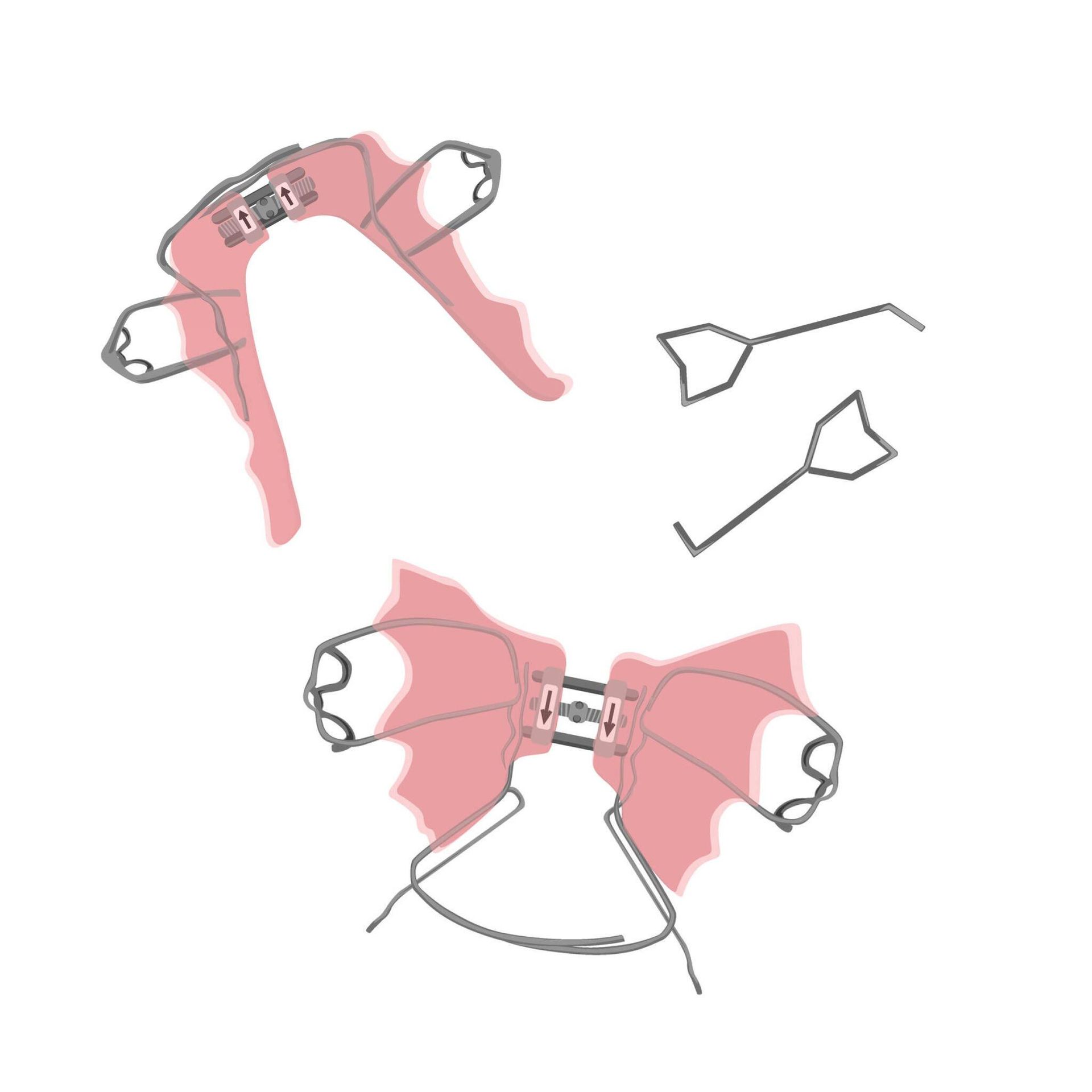
1. Palatal expanders: An orthodontic appliance that aims to widen a narrow palate and is used to create space for all of the permanent teeth; it fits in the roof of the mouth and gradually pushes the two halves of the jawbone apart. In situations involving cross bites or overly crowded teeth, the orthodontist may recommend the use of expanders. This device is mostly efficient during childhood or adolescence as the maxillary bones become harder to expand once puberty is reached.
2. Braces: The treatment of malocclusion and proper teeth alignment traditionally involves the use of braces. A variety of dental issues can be effectively corrected through the use of braces. Traditional braces are composed of brackets that are bonded to the teeth, along an archwire that securely connects these brackets. This combination enables the teeth to be properly aligned and straightened.

3. Clear aligners: Transparent and removable orthodontic devices that have recently gained significant popularity; they utilize CAD/CAM technology to digitally scan dental arches and fabricate transparent trays made of a strong plastic material to fit each individual's mouth. The treatment involves multiple sets of aligners, patients are required to wear each set for 7-10 days for a minimum of 22 hours per day to allow the teeth to gradually straighten and achieve the desired results. Clear aligner treatment is particularly suitable for individuals who cannot attend many appointments and prioritize aesthetics.

[1] “AOSocclusaloverview.Pdf.”
[2] Devi, Keisam, and Singh, “Malocclusion and Occlusal Traits among Dental and Nursing Students of Seven North-East States of India.”
[3] “AOSocclusaloverview.Pdf.”
[4] Devi, Keisam, and Singh, “Malocclusion and Occlusal Traits among Dental and Nursing Students of Seven North-East States of India.”
[5] “AOSocclusaloverview.Pdf.”
[6] “AOSocclusaloverview.Pdf.”
[7] Chu, Kennedy, and Hatzimanolakis, “Knowledge of Malocclusion Supports Comprehensive Dental Hygiene Care.”
[8] Devi, Keisam, and Singh, “Malocclusion and Occlusal Traits among Dental and Nursing Students of Seven North-East States of India.”
[9] Devi, Keisam, and Singh.
[10] Devi, Keisam, and Singh.
[11] Al-Hummayani, “Pseudo Class III Malocclusion.”
[12] Chu, Kennedy, and Hatzimanolakis, “Knowledge of Malocclusion Supports Comprehensive Dental Hygiene Care.”